|
GASTROSCHISIS |
ULTRASOUND (1-14) |
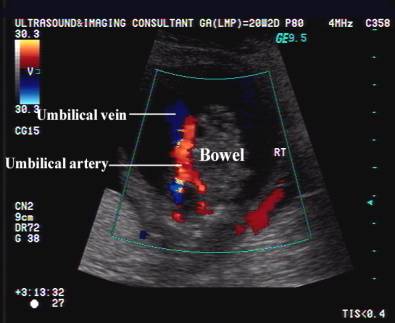
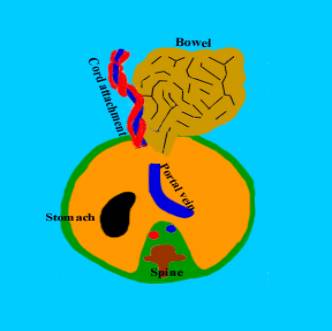
- Defect is adjacent to, and almost always to the right of the normal umbilical cord insertion. Left sided gastroschis has been reported but is rare.
|
|
|
- The defect is small (usually <2 cm) and involves the full thickness of the abdominal wall.
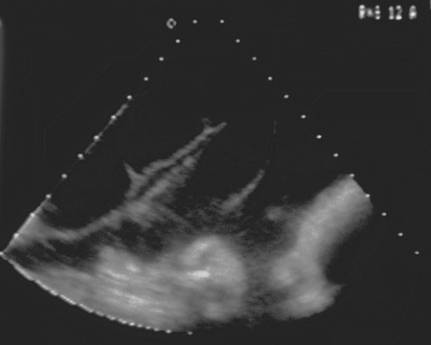
- Freely floating bowel loops outside the fetal abdomen (no limiting membranes).
|
|

- Bowel wall may be thickened (probably from exposure to fetal urine) (2) Meconium may be present in small amounts, in normal amniotic fluid, and this may further irritate exposed bowel (3,4). Langer et.al. (17) found that bowel wall thickening of >3 mm to be present in 42% of their gastroschisis fetuses, and was associated with an increase in time to initiate oral feeding, but the difference was not statistically significant.
|
|

|
|
|
|
|
|
|
|

- No peritoneal covering.
|
|
|
|
|
|



- Dilated intra or extraperitoneal bowel (a single cutoff value for bowel or subjective assessment of fetal bowel dilatation is impractical) (13). Workers have generally used >17 mm as bowel dilatation, however bowel dilatation of > 17 mm without postnatal complications are well reported (16).
|
|
- Small bowel extrusion occurs consistently (large bowel rarely extrudes)
- <3-5 cm defect, usually on the right side of the cord insertion.
- Normal insertion of the umbilical cord on the fetal abdomen.
- A small amount of skin is present between the defect and the umbilicus.
- Polyhydramnios may be present. A study by Japaraj et.al. (16) suggests that polyhydramnios is the only significant sonographic finding that was strongly predictive of severe bowel complications in the neonatal period. It is thought that the polyhydramnios may be a sign of severe bowel damage, and may be related to bowel atresia and / or decreased or absent bowel motility.
- No fetal ascites.
- Abuhamad et.al. (18) found Doppler velocimetry of the superior mesenteric artery and its branches to be minimally useful in predicting the postnatal prognosis when compared to bowel dilatation.
- Structurally normal fetal urinary tract may become functionally obstructed as increasing amounts of abdominal contents herniated through the defect. The fetal bladder may herniated through the defect (15) and appear as a large, fluid-filled cyst in the amniotic cavity. Hydronephrosis can also develop both in the presence and absence of bladder herniation. In either situation, the upper tract dilatation appears to resolve postnatally following repair of the abdominal wall defect.
- Table comparing gastroschisis,
omphalocele and umbilical cord hernia.
- Disappearing abdominal wall defects have been described (5-7).
- Pitfall – gastroschisis that is obvious at mid-trimester scanning may be difficult to perceive in the third trimester. Although the bowel loops are larger, they are located at a distance from the defect in the anterior abdominal wall. If the fetal back is facing anteriorly or if there is oligohydramnios, the omphalocele may be invisible.
- Closed gastroschisis – this occurs when there is a significant progressive narrowing of the abdominal wall defect around the prolaped bowel. This is very serious and may lead to midgut infarction and vansihing bowel ending in short bowel syndrome. It may be difficult to discriminate between relatively harmless bowel obstruction and obstruction caused by a closure with possible fatal consequences.. This may be suspected when there is persistent intra-abdominal dilatation in the third trimester, especially if the dilatation is newly developed.
REFERENCES |
- Perrela RR, Ragavendra N, Tessler FN et.al. Fetal abdominal wall mass on prenatal sonography: gastroschisis vs omphalocele. AJR 1991;157:1065-1068.
- Kluk P, Tibboel D, Van Der Kamp et.al. The effect of fetal urine on the development of the bowel in gastroschisis. J Pediatr Surg 1983;18:47-50.
- Kizilcan F,
- Fenton AN, Steer CM. Fetal distress. Am J Obstet Gynecol 1962;83:354.
- Finley bE, Burlbaw J, Bennett TL et.al. Delayed return of the fetal midgut to the abdomen resulting in volvulus, bowel obstruction and gangrene of the small bowel. J Ultrasound Med 1992;11:233.
- Bromley B, Benacerraf BR. Transient omphalocele. J Ultrasound Med 1993;12:688.
- Bromley B, Shamberger RC, Benacerraf B. An unusual outcome for a fetus with gastroschisis. J Ultrasound Med 1995;14:69-72.
- Emanuel PG, Garcia GI, Angtuaco TL. Prenatal detection of anterior abdominal wall defects with US. Radiographics 1995;15:517-530.
- Lenke RR, Persutte WH. Nemes J. Ultrasonographic assessment of intestinal damage in fetuses with gastroschisis: IS it of any clinical value. Am J Obstet Gynecol 1990;163:995.
- Dinatti LA, Meagher DP,
- Bond SJ, Harrison MR, Filly RA et.al. Severity of intestinal damage in gastroschisis. J Pediatr Surg 1988;23:520.
- Sipes SL, Weiner CP, Williamson RA et.al. Fetal gastroschisis complicated by bowel dilatation: An indication for imminent delivery? Fetal Diagn Ther 1990;5:100.
- Babcock CJ, Hedrick MH, Goldstein RB et.al. Gastroschisis: Can sonography of fetal bowel accurately predict postnatal outcome. J Ultrasound Med 1994;13:701-706.
- Paidas MJ, Crombleholme TM, Robertson FM. Prenatal diagnosis and management of the fetus with an abdominal wall defect. Semin Perinatol 1994;18:196.
- Reiss RE, Landon MB, Jayanthi VR, Caniano K, Mutabagani K, O’Shaughnessy RW. Functional urinary tract obstruction developing in fetuses with isolated gastrochisis. Ultrasound Obstet Gynecol 2000;15:194-198.
- Japaraj RP, Hockey R, Chan FY. Gastroschisis: can prenatal sonography predict neonatal outcome. Ultrasound Obstet Gynecol 2003;21:329-333.
- Langer JC, Khanna J, Caco C et.al. Prenatal diagnosis of gastroschisis: dvelopment of objective sonographic criteria for predicting outcome. Obstet Gynecol 1993;81:53-56.